The year of 2018 has been a medically challenging one for this retired internal medicine physician. When people ask me how I am feeling, I always just say that I am experiencing medicine from the other side of the check in desk. I have been retired for over 10 years and no longer proceed through those secret corridors where all the mysteries of our medical care take place. At now almost 75 years of age, I guess it is not unusual to need the help of my former colleagues in medical care.
 My most recent encounters have centered around new onset atrial flutter. On August 14, I was just relaxing on a Wednesday afternoon, looking at my emails, sitting in my upholstered chair in our living room. My husband was contentedly watching the afternoon news. Suddenly I felt some flip flopping in my chest. At first I thought it was just some early atrial beats which I tend to get quite often. But in a moment I knew this was different. I quickly found my carotid pulse and it was very rapid. I tried to count it and came up with a heart rate in the 140s. I tried a cough, and also held my breath and bore down (the Valsalva maneuver) but this did nothing. It didn't take me long to realize that I would have to go to the emergency room. I was tolerating this rapid rate OK. I was not short of breath or dizzy, no chest pain, but it certainly was not comfortable to have the heart pounding in my chest as it was. I told Amos he would have to take me to the ER at the Grafton hospital where I usually get my care. It was now about 4:30 in the afternoon. After check in, assessment by nurse and doctor and an EKG, I was diagnosed with typical atrial flutter with a rate of about 125. Blood work showed no evidence of electrolyte abnormalities, thyroid hyperactivity, or acute coronary occlusion or myocardial infarction. In other words, no obvious serious cause. Apparently intravenous diltiazem which is used to convert this abnormal rhythm to normal sinus rhythm had been in short supply and none was to be had in the pharmacy, so I was treated with an alternative calcium channel blocker, verapamil, and in about an hour and a half I converted to normal rhythm. The ER doc consulted the electrophysiologist on call and I was discharged home on oral diltiazem to try to prevent this from happening again. I was told to follow up with the electrophysiologist for an outpatient cardiac workup.
My most recent encounters have centered around new onset atrial flutter. On August 14, I was just relaxing on a Wednesday afternoon, looking at my emails, sitting in my upholstered chair in our living room. My husband was contentedly watching the afternoon news. Suddenly I felt some flip flopping in my chest. At first I thought it was just some early atrial beats which I tend to get quite often. But in a moment I knew this was different. I quickly found my carotid pulse and it was very rapid. I tried to count it and came up with a heart rate in the 140s. I tried a cough, and also held my breath and bore down (the Valsalva maneuver) but this did nothing. It didn't take me long to realize that I would have to go to the emergency room. I was tolerating this rapid rate OK. I was not short of breath or dizzy, no chest pain, but it certainly was not comfortable to have the heart pounding in my chest as it was. I told Amos he would have to take me to the ER at the Grafton hospital where I usually get my care. It was now about 4:30 in the afternoon. After check in, assessment by nurse and doctor and an EKG, I was diagnosed with typical atrial flutter with a rate of about 125. Blood work showed no evidence of electrolyte abnormalities, thyroid hyperactivity, or acute coronary occlusion or myocardial infarction. In other words, no obvious serious cause. Apparently intravenous diltiazem which is used to convert this abnormal rhythm to normal sinus rhythm had been in short supply and none was to be had in the pharmacy, so I was treated with an alternative calcium channel blocker, verapamil, and in about an hour and a half I converted to normal rhythm. The ER doc consulted the electrophysiologist on call and I was discharged home on oral diltiazem to try to prevent this from happening again. I was told to follow up with the electrophysiologist for an outpatient cardiac workup.
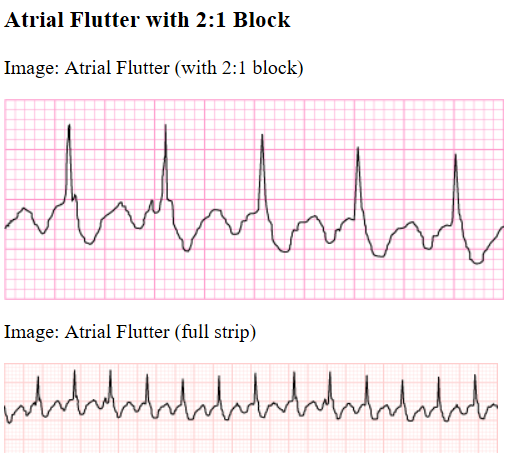
Here you deserve a little explanation about what atrial flutter is. Many people have probably heard of atrial fibrillation, one of the most common heart electrical rhythm disturbances. Well, atrial flutter is a little different. As opposed to atrial fibrillation which is totally irregular with aberrant electrical impulses coming from mostly the left atrium but also some from the right atrium, originating like fireworks through out those two upper chambers of the heart, atrial flutter is a rapid regular heart beat which usually occurs in the right atrium only and consists of a circular electrical impulse that occurs at such a rate that it can keep restimulating the same tissue over and over again in what is called a reentrant rhythm. By the time the impulse gets back to its origin, that electrical tissue of the heart has repolarized and is set off again in a repeating pattern. Usually the rate is from 250 to 300 atrial beats per minute. Not all these beats are able to get through to make the ventricles of the heart contract. There is usually a 2 to 1, a 3 to 1, or a 4 to 1 block so that the ventricular rate is half, 1/3, or 1/4 the rate of the atria. In my case, with a rate of 125, I had a 2 to 1 block at the time the EKG was taken. Atrial flutter is usually not a life threatening rhythm immediately, but there are two risks that develop if allowed to continue. When the atria are not beating properly either irregularly or too rapidly blood clots tend to form within the heart and can break off and go elsewhere in the body, most damaging to the brain causing a stroke, or to the heart itself causing a heart attack. Secondly if the rhythm is too rapid for long periods of time, the heart tires and begins to go into heart failure. Therefore ideally flutter needs to be converted to a normal slower rhythm or at the very least to a slower flutter rate and blood thinners need to be used to prevent those blood clots from forming.
Two weeks later, I was having a lot of irregularity in my pulse. I was not having the regular rapid pulse of flutter, but instead normal rate but very irregular beats. The concern with flutter is that it can be mixed with episodes of atrial fibrillation which carries a higher risk of complicating stroke. I called my primary care doctor's office to get an appointment and couldn't get in with her but another previous partner of mine agreed to see me. Well, of course, on the way driving to the appointment, the irregularities stopped and taking my pulse, I knew I was in sinus rhythm again. My former partner correctly ordered a Holter monitor to be set up to see if we could catch these episodes of irregularities and further diagnose what they were. This was a 48 hour monitoring and I was able to drive right over to Grafton hospital and get hooked up with this monitor.
Here you deserve a little explanation about what atrial flutter is. Many people have probably heard of atrial fibrillation, one of the most common heart electrical rhythm disturbances. Well, atrial flutter is a little different. As opposed to atrial fibrillation which is totally irregular with aberrant electrical impulses coming from mostly the left atrium but also some from the right atrium, originating like fireworks through out those two upper chambers of the heart, atrial flutter is a rapid regular heart beat which usually occurs in the right atrium only and consists of a circular electrical impulse that occurs at such a rate that it can keep restimulating the same tissue over and over again in what is called a reentrant rhythm. By the time the impulse gets back to its origin, that electrical tissue of the heart has repolarized and is set off again in a repeating pattern. Usually the rate is from 250 to 300 atrial beats per minute. Not all these beats are able to get through to make the ventricles of the heart contract. There is usually a 2 to 1, a 3 to 1, or a 4 to 1 block so that the ventricular rate is half, 1/3, or 1/4 the rate of the atria. In my case, with a rate of 125, I had a 2 to 1 block at the time the EKG was taken. Atrial flutter is usually not a life threatening rhythm immediately, but there are two risks that develop if allowed to continue. When the atria are not beating properly either irregularly or too rapidly blood clots tend to form within the heart and can break off and go elsewhere in the body, most damaging to the brain causing a stroke, or to the heart itself causing a heart attack. Secondly if the rhythm is too rapid for long periods of time, the heart tires and begins to go into heart failure. Therefore ideally flutter needs to be converted to a normal slower rhythm or at the very least to a slower flutter rate and blood thinners need to be used to prevent those blood clots from forming.
Two weeks later, I was having a lot of irregularity in my pulse. I was not having the regular rapid pulse of flutter, but instead normal rate but very irregular beats. The concern with flutter is that it can be mixed with episodes of atrial fibrillation which carries a higher risk of complicating stroke. I called my primary care doctor's office to get an appointment and couldn't get in with her but another previous partner of mine agreed to see me. Well, of course, on the way driving to the appointment, the irregularities stopped and taking my pulse, I knew I was in sinus rhythm again. My former partner correctly ordered a Holter monitor to be set up to see if we could catch these episodes of irregularities and further diagnose what they were. This was a 48 hour monitoring and I was able to drive right over to Grafton hospital and get hooked up with this monitor.
The Holter monitor showed many PVCs, premature ventricular beats this time. I noticed these while being on the Holter monitor, mostly when my pulse slowed below 60. I even jogged in place while on the Holter to see if the elevated pulse of exercise would suppress the PVCs and that is exactly what happened. My elcectrophysiologist agreed with my thought to reduce the dose of diltiazem slightly because that does slow the heart rate. I was having a resting heart rate sometimes of 50. I did OK for a while but then I had a second episode of atrial flutter and again had to go to the ER. IV meds again stopped the episode but now a decision would have to be made. I could just always go to the ER when this happened, but my electrophysiologist suggested a cardiac ablation. This is a procedure done with a catheter placed in the femoral vein in the groin which is then fed upwards to the right atrium where a quite complicated computer mapping system pinpoints where this flutter electric impulse starts. In the case of typical flutter, there are very few variations in this site. Then electrical burns are placed in a circle around this area to prevent these impulses from propagating to the rest of the atrium and triggering that rapid rentry flutter pattern. I must say that as a doctor entering that ablation laboratory, I was amazed at the equipment, at a whole wall of computer screens and about 7 people monitoring, serving as operative assistants, imaging and ultrasound technicians, anesthesiolgist, computer screen technicians, and personal nursing caregivers. Wow! A wonderful example of where medicine has arrived. Everything went well, and after about 6 hours of rest to let the femoral vein site close more securely, I was released to go home. All over. No further atrial flutter. The only thing I object to is the fact that the electrophysiologist still thinks I am high risk for atrial fibrillation since there was a 20 beat run of it on my Holter monitor. Also my left atrium is slightly to moderately dilated and this enlargement is one of the preceding hallmarks of atrial fibrillation risk. This means I am on blood thinning medications chronically to prevent stroke. The medications used for thinning the blood to prevent clots is better than that used in the past, which was actually rat poison, or warfarin. That med required weekly to monthly blood monitoring and even a special diet. Eliquis is better, doesn't require either of these. So a new med to my list and I am on about my business. No other losses of function or activities. Yey!

